The healthcare workers (HCWs) have been on the frontline in combating the pandemic and were prioritized for vaccination when COVID-19 vaccines became available.
Although vaccines effectively prevent infection in most cases, some cases of post-vaccination infections have been reported, raising concerns about vaccine efficacy. This study investigated the efficacy of COVID-19 vaccines in preventing and reducing the severity of post-vaccination infections (PVI) among HCWs.
Methods: This observational study examined 28342 vaccinated HCWs with SARS-CoV-2 (symptomatic severe acute respiratory syndrome coronavirus 2)infections during the initial five months of vaccination (January 16-June 15, 2021). They worked at 43 Apollo Group hospitals in 24 Indian cities. PVI was investigated after recombinant ChAdOx nCOV-19 (Recombinant) or the whole virion inactivated Vero cell vaccines were administered. Various parameters were evaluated such as age, sex, time to infection, type of vaccine, infections after a single and two doses, monthly and regional case distribution, clinical severity of infection, hospitalization and intensive care unit (ICU)
requirement, and death.

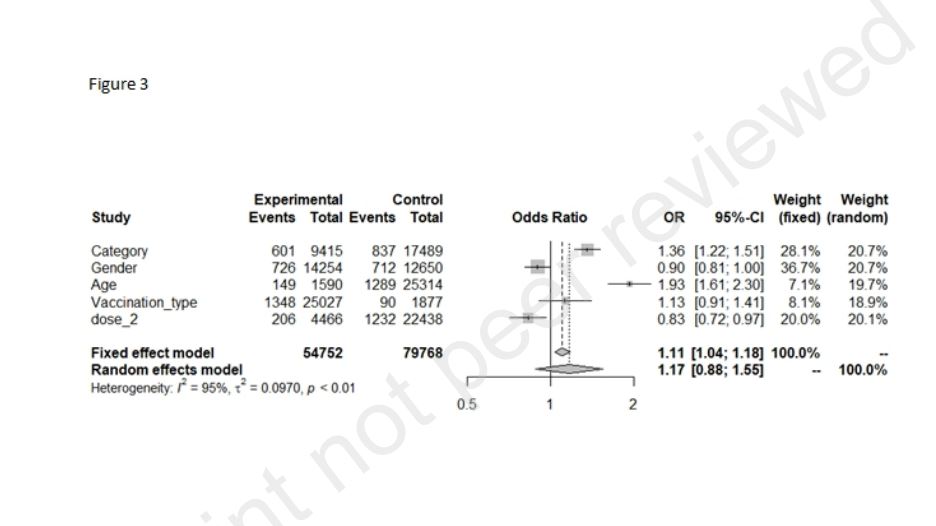
Findings: Symptomatic PVIs occurred in a low percentage of vaccinated cohorts (5⸱07%, p<0⸱001), and these were predominantly mild and did not result in hospitalization, ICU admissions (p<0⸱0001), or death. Both vaccines provided similar protection, with PVIincidences of 5⸱11% and 4⸱58%, following ChAdOx nCOV-19 (Recombinant) and the whole virion inactivated Vero cell vaccines, respectively (p<0⸱001). Nursing and Clinical staff and cohorts>50 years significantly contracted more infections(p<0⸱001 and p=0⸱001, respectively). Two-dose vaccination has significantly lower odds of developing PVI (0.83, 95%CI – 0.72 to 0.97). Maximum infections
occurred during the peak of the second COVID-19 wave from mid-April to May 2021 (p<0⸱001). No
This preprint research paper has not been peer reviewed. Electronic copy available at: https://ssrn.com/abstract=3889352 Preprint not peer reviewed 4 significant difference existed in the infection between sex, vaccine type, and the number of vaccine doses received (p≥0⸱05).
Interpretation: PVIoccurred in a small percentage of HCWs. Vaccination protected them
significantly from the infection but also severe disease.
Introduction
The coronavirus disease (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that is highly contagious, has spread globally since it was first detected in December 2019. India has experienced a significant resurgence of the virus during the second wave of the pandemic, which had its peak in April and May 2021. The only hope for effective control and mitigation of this pandemic are effective and large-scale vaccination efforts. Several vaccines for preventing SARS-CoV-2 infection have been developed in many countries, including India, at a phenomenal speed.
The Government of India first permitted the clinical use of two types of vaccines, namely ChAdOx nCOV-19 (Recombinant) coronavirus vaccine (recombinant) and a whole virion inactivated Vero cell vaccine.3, 4, 5 A mass vaccination program was implemented in India in multiple phases beginning January 16, 2021. The first phase of vaccinations included healthcare workers (HCWs), people aged over 60 years, and people aged over 45 years with
significant medical comorbidities. They were administered one of the two approved vaccines at vaccination centers.

The ChAdOx nCOV-19 (Recombinant) vaccine is currently the most commonly used in India. It is a viral vector vaccine manufactured by modifying the chimpanzee adenovirus ChAdOx and was developed by AstraZeneca and Oxford University (UK). The vaccine is manufactured and sold in India by the Serum Institute, Pune. Its reported efficacy for preventing symptomatic COVID-19 is 76⸱0% three weeks after the first dose and 81⸱3% after the second dose. The other approved vaccine in India is a whole virion inactivated Vero cell vaccine, developed by Bharat Biotech (Hyderabad, India) in collaboration with ICMR and the National Institute of Virology. It was
approved by the GOI for emergency use in the prevention of COVID-19 after a successful phase-2 trial. It has demonstrated 78% efficacy in preventing mild, moderate, and severe COVID-19 cases and has demonstrated efficacy in preventing infection by mutant and heterogeneous viral strains of SARS-COV-2. It is pending approval by the World Health Organization (WHO).
HCWs have been on the frontline of efforts to combat the pandemic and were thus prioritized for vaccination when COVID-19 vaccines became available. It was essential to prioritize vaccination of HCWs because they have a greater occupational risk of becoming infected. Additionally, infected HCWs reduce the number of healthy HCWs available at a given time, thereby reducing the availability of their much-needed services during a critical time. Furthermore, HCWs present a risk of transmitting SARS-CoV-2 infection to their family members and the general public.7
Although it is now widely known that the available COVID-19 vaccines are safe and effective, there have still been concerns about their efficacy and possible side effects.
Recently, some cases of postvaccination infections (PVIs) have been reported.The Center for Disease Prevention and Control (CDC) has defined the breakthrough infections (BTIs) when the PVI occurs two weeks after the
second dose of COVID-19 vaccination.
Thus, this study aimed to investigate the efficacy of COVID-19 vaccines in preventing and reducing the severity of PVIs in a large cohort of HCWs employed at Apollo Group hospitals, the largest chain of hospitals in India, after they received the vaccines.

Materials and Methods
This retrospective observational cohort study was conducted among HCWs worked at various Apollo Group hospitals across India.This study was approved by an Ethical Institutional Committee (EIC), and a consent waiver was given by the EIC. We collated and analyzed hospital data of HCWs obtained from the Medical Records Departments and Human Resource Departments of the hospitals included in this study. The 5-month study period was from January 16, 2021, to June 15, 2021.
We assessed records of all HCWs who received COVID-19 vaccination and developed PVIs. These HCWs were doctors, nurses, paramedics, administrative staff, and support staff. Two types of vaccines were administered to these cohorts: ChAdOx nCOV-19 Recombinant (CovishieldTM, Serum Institute, India) and a whole virion inactivated Vero cell vaccine (CovaxinTM, Bharat Biotech, India) depending on the availability of each vaccine at different vaccination centers.
We divided PVIs into two groups: (A) PVIs following full vaccination (FV; two doses) and (B) PVIs following partial vaccination (PV; one dose).In addition, the Breakthrough Infections (BTI) was considered when the PVI occurred after two weeks of the two vaccine doses.
The inclusion criteria of this study were the participants working at an Apollo Group hospital, receipt of COVID-19 vaccination, and later acquisition of SARS-CoV-2 PVI. Only symptomatic COVID19 cases with a positive reverse transcription-polymerase chain reaction (RT-PCR) test result were included. We excluded all participants with asymptomatic PVIs (due to resource constraints and logistic reasons), non-vaccinated HCWs, and those with negative RT-PCR test results.
The data was collected, analyzed, and compared for various parameters such as age, sex, time to PVI, type of vaccine, PV or FV status, monthly and regional case distribution, clinical severity of PVI, hospitalization requirements, intensive care unit (ICU) need, and death. Multiple bivariate analyses were performed to assess the relationship between candidate variables and outcomes. Statistical analyses were performed using IBM-SPSS version 20TM (IBM, USA). A chi-squared test was performed to determine the association among various categorical variables. The Z-test for differences between proportions was used as appropriate, and relative risks and 95% confidence
intervals (CIs) were calculated. Statistical significance was defined by p-values <0⸱05.
We did not receive any funding from any source, for conducting this study or for data collection and
analysis.
Figure legends:
Figure 1: Total vaccine doses administered (blue) and the incidence of post-vaccination infections
(red)
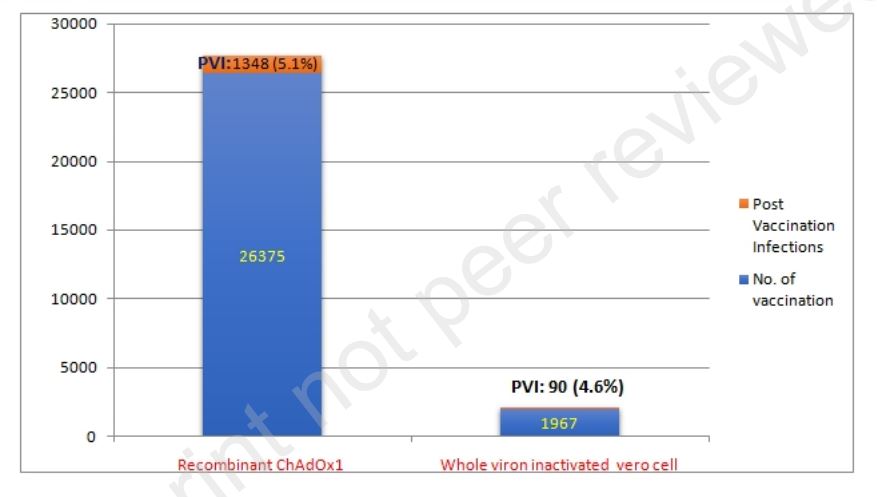
Figure 2: Pattern of post-vaccination infections in various age groups
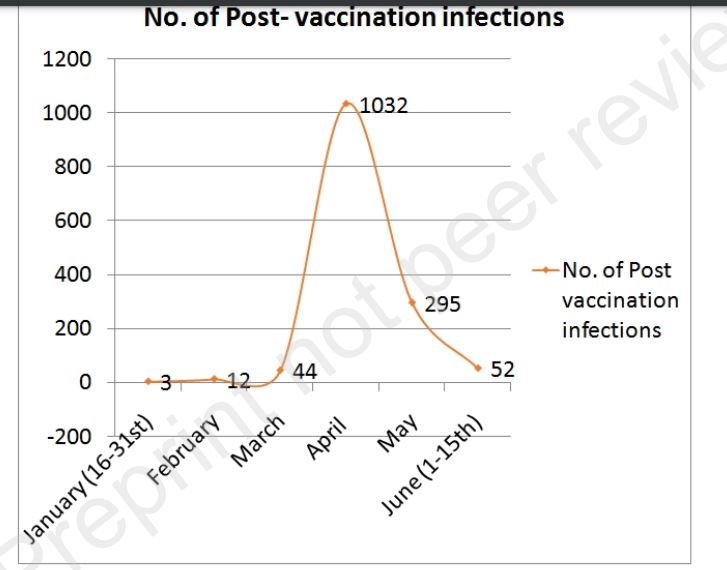
Figure 3: Monthly distribution of post-vaccination infections in the study